Need to Talk to Someone?
What Is Generalised Anxiety Disorder?
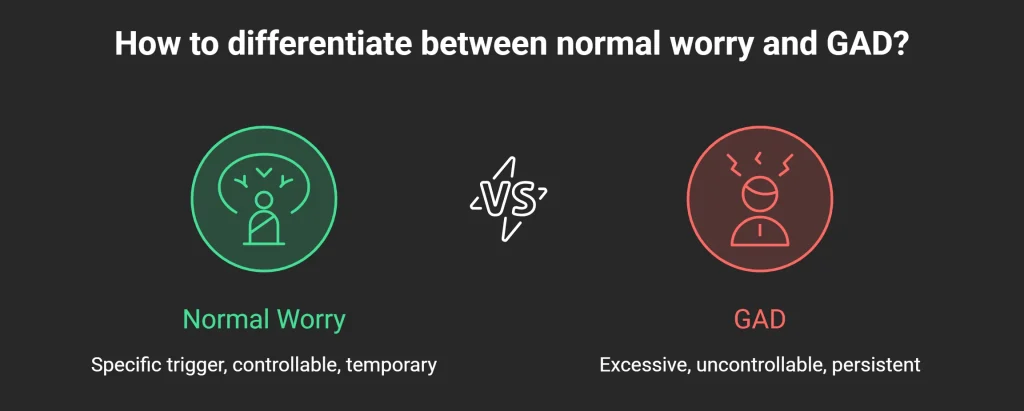
How GAD Differs from Normal Worry
Symptoms of GAD: What to Look For
Psychological Symptoms
- Difficulty concentrating, often described as a mind that feels “full” or constantly distracted
- Irritability that seems disproportionate to the immediate situation
- A persistent sense that something bad is about to happen, even without a specific threat
- Difficulty making decisions, driven by fear of choosing wrongly
- Seeking excessive reassurance from others, which provides only brief relief
Physical Symptoms
Sleep Disturbance
What Causes GAD?
Genetic and Biological Factors
Psychological Factors
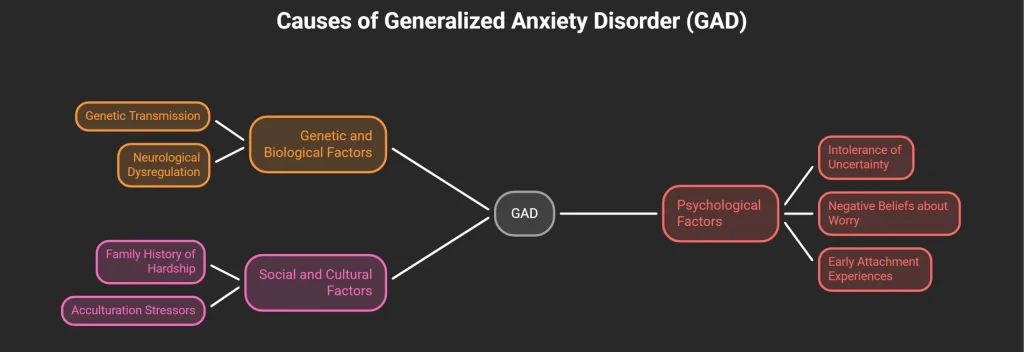
Social and Cultural Factors
How GAD Is Diagnosed
Effective Treatments for GAD
Cognitive Behavioural Therapy for GAD
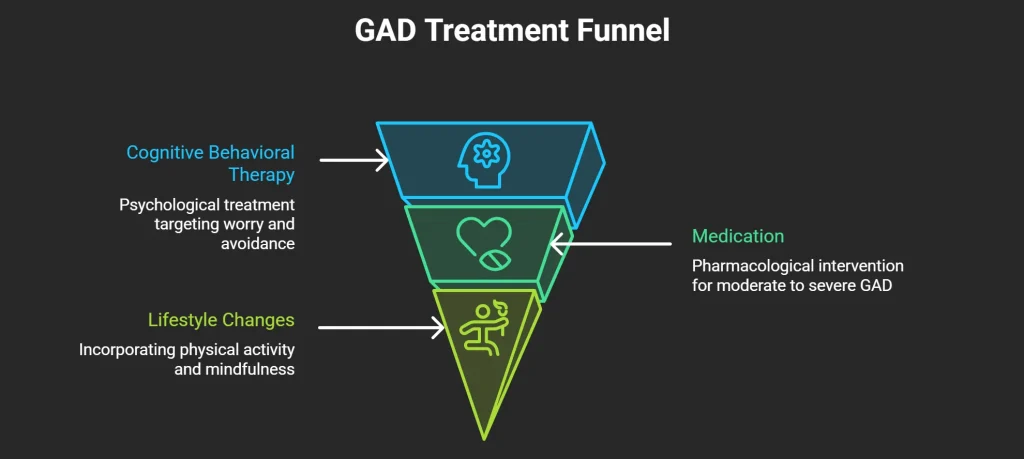
Medication
Lifestyle and Adjunctive Approaches
When to Seek Professional Help
Frequently Asked Questions
The core symptom is excessive, persistent worry about multiple areas of life — health, finances, family, work — that is difficult to control and present on most days for at least six months. This is accompanied by at least three physical or psychological symptoms, which may include restlessness, fatigue, difficulty concentrating, irritability, muscle tension, and disturbed sleep. Many people with GAD also experience physical complaints such as headaches, digestive problems, and palpitations, which are direct effects of chronic physiological arousal.
The key differences are duration, intensity, and controllability. Normal anxiety is proportionate to a real threat and eases when the situation resolves. In GAD, the worry is excessive relative to the actual risk, spans multiple topics simultaneously, is present on most days for months or years, and feels very difficult to stop even when you want to. If your worry is interfering with your sleep, your work, or your relationships consistently, it warrants a proper assessment rather than continued self-management.
For some people, GAD symptoms fluctuate — they may reduce during stable periods and worsen under stress. However, without treatment, the underlying patterns that drive GAD (particularly intolerance of uncertainty and cognitive avoidance) tend to persist. Research consistently shows that structured treatment, particularly CBT, produces more sustained improvement than the condition resolving untreated. Waiting for it to pass on its own often means years of unnecessary suffering, and the condition can worsen if left unaddressed.
Anxiety disorders are common globally, and South Asian communities face specific risk factors that increase vulnerability: intergenerational transmission of anxious coping patterns, migration and acculturation stress, family pressures around performance and reputation, and significant stigma around seeking psychological help. Research published in Transcultural Psychiatry has found elevated rates of anxiety among South Asian diaspora populations in Western countries. Within India, NIMHANS data suggests anxiety disorders are significantly underdiagnosed due to the predominance of physical symptom presentation.
Yes. Oppam offers online counselling in Malayalam, Tamil, and English, with therapists who are trained in evidence-based approaches for anxiety disorders. Being able to work in your first language matters clinically — it allows for more precise expression of emotional experience and reduces the effort of self-monitoring in a second language. Sessions are conducted online, making them accessible regardless of where you are located.
This varies depending on severity and the approach used. A standard course of CBT for GAD typically involves 12 to 20 sessions, with many people experiencing significant improvement within the first six to eight sessions. Medication, if used, generally requires four to six weeks before full effects are felt. Some people benefit from a shorter course of therapy focused on specific skills, while others find ongoing support more useful. Your therapist will work with you to set a realistic plan based on your individual presentation.
Yes, there is a strong association. According to the APA, a significant proportion of people diagnosed with GAD also meet the criteria for a depressive disorder at some point. The two conditions share some neurobiological features and tend to worsen each other: chronic anxiety is exhausting and demoralising, which can tip into depression, while depression reduces the cognitive and emotional resources needed to manage anxiety. When both are present, treatment needs to address both, which is why accurate diagnosis matters.
External Resources
- World Health Organisation (WHO) — Global prevalence data: anxiety disorders affect 301 million people (2022 Mental Health Atlas)
- American Psychiatric Association / DSM-5 — Diagnostic criteria for GAD, panic disorder, social anxiety disorder
- JAMA Psychiatry — Meta-analysis of CBT efficacy for anxiety disorders; equivalence of online and in-person delivery
- International Journal of Social Psychiatry — Acculturation stress and elevated anxiety/depression rates in South Asian diaspora populations in the UK
- Indian Journal of Psychiatry — Somatisation of psychological distress in Indian clinical populations
- NICE (UK) — Clinical guidelines for the treatment of GAD; first-line recommendations for SSRI/SNRI use
- Transcultural Psychiatry — Acculturation stress and elevated GAD rates in South Asian migrant populations