Postpartum Depression Gulf Mothers?.. The baby is healthy. The husband has taken a week off work. The apartment is clean, the relatives have sent gifts, and everyone who calls says the same thing: you must be so happy. And she tries to feel it. She looks at the baby and waits for the love to arrive in the form she expected, overwhelming, certain, unmistakable. But what she feels instead is a blankness that frightens her, a heaviness behind the eyes, an exhaustion that sleep does not touch. She does not feel like herself. She does not feel like anyone.
She says nothing. Because what kind of mother feels this way? What would her mother-in-law think? What would her husband think? The cultural expectation in Kerala and across the Gulf diaspora is that new motherhood is a time of joy — the family has grown, God has been good, there is nothing to be unhappy about. So she performs the happiness and carries the rest privately, alone in a Gulf apartment far from everyone who knows her well.
Need to Talk to Someone?
Book a private online session with a licensed therapist
Postpartum depression is not a failure of love or gratitude. It is a clinical condition with a well-understood biological basis, a clear set of symptoms, and effective treatments. According to the World Health Organisation, it affects approximately 10 to 15 per cent of mothers following childbirth globally — one in seven. Among South Asian women in the Gulf diaspora, where specific structural and cultural risk factors converge, the true prevalence may be higher. And because of the stigma and the silence, the majority of those women receive no professional support.
What Postpartum Depression Actually Is
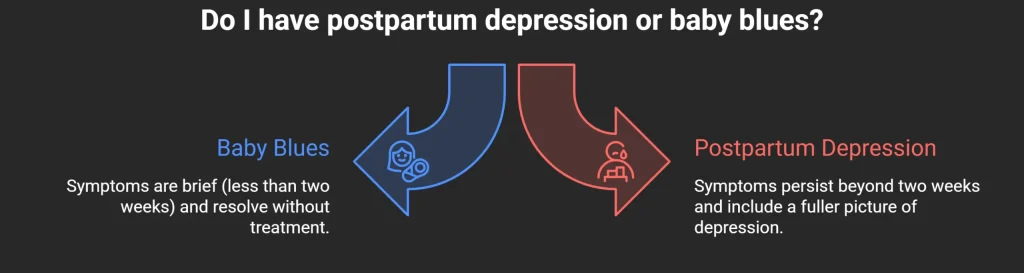
Postpartum depression (PPD), also called postnatal depression, is a depressive episode that begins within four weeks of childbirth, though it can onset up to a year after delivery in some presentations. It is distinct from the baby blues — the brief period of tearfulness, mood fluctuation, and emotional sensitivity that affects up to 80 per cent of new mothers in the first week after birth and typically resolves within two weeks without treatment. If the low mood, flatness, or distress persists beyond two weeks and is accompanied by the fuller symptom picture of depression, what is present is postnatal depression rather than the normal hormonal adjustment of the immediate postpartum period.
The DSM-5 classifies postpartum depression as a Major Depressive Episode with peripartum onset, with the same diagnostic criteria as depression in other contexts — persistent low mood or loss of interest, fatigue, sleep disturbance beyond what is explained by the newborn’s needs, appetite changes, difficulty concentrating, feelings of worthlessness or excessive guilt, and in severe cases, thoughts of self-harm or thoughts of harming the baby. The last of these — intrusive thoughts about the baby’s safety — are a particularly frightening symptom that causes enormous shame and is almost never disclosed without a directly supportive clinical context.
The biological drivers of PPD are well established. The dramatic drop in oestrogen and progesterone following delivery — levels that had been elevated throughout pregnancy — produces neurochemical changes analogous to those seen in other depressive episodes. These are compounded by sleep deprivation, physical recovery from labour, and the sudden transition in identity and role that new parenthood represents. The condition is not caused by weakness, insufficient love for the baby, or inadequate faith. It has a clear physiological mechanism.
Why Gulf-Based South Asian Mothers Are Particularly Vulnerable
While postpartum depression occurs across all cultures and demographics, Gulf-based South Asian mothers face a specific convergence of risk factors that elevates both the likelihood of developing the condition and the barriers to having it recognised and treated.
Geographical Isolation From Family Support
In Keralite and South Asian cultural tradition, the postpartum period — typically the first forty days — is a time of intensive family support. The new mother’s own mother, mother-in-law, sisters, and aunts converge to take over the household, care for the baby, and care for the mother: feeding her specific foods believed to aid recovery, ensuring she rests, managing the household so she does not have to. This system, whatever its imperfections, provides real structural support during one of the most physically and emotionally demanding periods of a woman’s life.
In the Gulf, this system is often entirely absent. The new mother is in an apartment in Dubai or Sharjah, potentially thousands of miles from her family. A mother or mother-in-law may visit for four to six weeks, which helps enormously, but then leaves. What remains is a woman who is managing a newborn, often largely alone, in a country that is not her own, without the dense support network her cultural tradition assumes will be present.
Research published in Archives of Women’s Mental Health has consistently identified social isolation as one of the strongest predictors of postpartum depression, with the strength of the relationship between isolation and PPD comparable to other well-established risk factors including a prior history of depression and significant life stressors. For Gulf NRI mothers, isolation is not an individual characteristic but a structural condition of their situation.
The Pressure to Perform Maternal Joy
South Asian cultural expectations around new motherhood are specific and demanding. The new mother is expected to be visibly happy, physically recovered quickly, breastfeeding successfully, managing the baby competently, and present for the needs of her husband and extended family — all simultaneously. The cultural frame does not provide much space for admitting that the reality feels different from the expectation.
The consequence is what clinicians call the masked presentation of postnatal depression: the mother performs functioning and contentment while carrying significant depression privately. She presents well on the phone calls home, manages the baby’s visible needs, and endures the rest without disclosure. The gap between performance and internal experience is exhausting, and the sustained effort of maintaining it worsens the depression it conceals.
In clinical practice with South Asian women, one of the most common statements made in a first postpartum therapy session is some version of: “I thought I was the only one who felt this way.” The combination of cultural expectation and social isolation produces an experience of complete uniqueness that compounds the shame and prevents disclosure.
The Breastfeeding Pressure
In Gulf-based South Asian communities, breastfeeding is not simply a feeding choice — it carries significant cultural and moral weight. The mother who cannot breastfeed successfully, or who finds breastfeeding painful, exhausting, or emotionally difficult, may experience this as a personal failure compounded by family pressure and cultural expectation. Breastfeeding difficulties are consistently identified in clinical literature as a risk factor for postpartum depression, and the cultural pressure that surrounds breastfeeding in South Asian communities amplifies this risk considerably.
What Postpartum Depression Looks Like: Symptoms in Detail
The standard symptom list for PPD mirrors the depression symptom criteria, but the way these symptoms present in the context of new motherhood has specific features that are important to understand.
Difficulty Bonding With the Baby
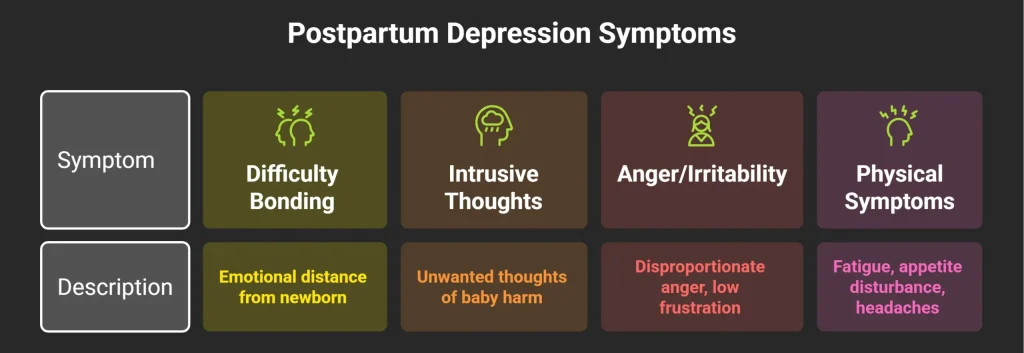
One of the most distressing and least discussed symptoms of postpartum depression is difficulty forming or feeling the expected emotional connection with the newborn. The mother may care for the baby competently — feeding, changing, holding — while feeling an emotional distance she does not understand and cannot discuss. She expected the love to be immediate and overwhelming. What she experiences is a flat, dutiful care without the warmth she anticipated.
This is a symptom. It is not evidence that she does not love her child, that she is a bad mother, or that she should not have had the baby. It is a neurobiological consequence of depression interfering with the emotional systems involved in attachment and bonding. It responds to treatment. The bond that feels absent during PPD typically establishes fully once the depression is addressed.
For South Asian mothers in the Gulf, this symptom is almost never disclosed to family because the shame it would produce is perceived as unsurvivable. It is disclosed to therapists, and even then only when the therapeutic relationship has established sufficient safety.
Intrusive Thoughts
A proportion of women with postpartum depression experience intrusive thoughts unwanted, involuntary mental images or thoughts, often about harm coming to the baby. A mother might have a sudden image of the baby falling, or an intrusive thought about what could happen during a bath. These thoughts are profoundly distressing and almost always produce intense shame and fear: “What kind of mother thinks this?”
Clinically, intrusive thoughts in the context of PPD are ego-dystonic — they are completely contrary to the person’s actual wishes and values. They are produced by the anxiety and hypervigilance that accompanies postnatal depression, not by any genuine intent to harm. They are a symptom, not a reflection of character. They are also highly treatable. But because they are so rarely disclosed, they are often suffered in complete silence for months.
Anger and Irritability
As with depression in other contexts, postpartum depression does not always present as sadness. Irritability, low frustration tolerance, anger that seems disproportionate to the trigger — these are common presentations, particularly in the context of sleep deprivation, physical recovery, and the relentless demands of a newborn. A mother who snaps at her husband, feels rage when the baby will not settle, or finds herself overwhelmed by what seem like small demands may not recognise this as depression. Her family may not recognise it either — they may attribute it to hormones, to tiredness, to her personality.
Physical Symptoms
Postpartum depression produces the same physical symptom profile as depression in other contexts: persistent fatigue that goes beyond what the disrupted sleep of new parenthood explains, appetite disturbance, headaches, and general physical heaviness. In Gulf-based South Asian mothers who may not have access to a trusted GP or who do not want to disclose psychological distress to a local doctor, these physical symptoms may go uninvestigated for extended periods.
The Role of the Husband and Extended Family
Postpartum depression is not solely a mother’s experience. It affects the marital relationship, the family system, and sometimes the father directly — paternal postnatal depression is a recognised condition affecting approximately 10 per cent of fathers following childbirth, according to research published in JAMA Psychiatry.
For Gulf-based Keralite families, the husband is often the only adult consistently present in the household. His capacity to recognise the signs of PPD, to respond supportively rather than with confusion or frustration, and to facilitate access to professional support is clinically significant. Husbands who dismiss the symptoms as hormonal, who express frustration with their wife’s emotional state, or who are themselves struggling with the adjustment to parenthood can inadvertently worsen the conditions that maintain PPD.
The most useful things a husband can do are: take the symptoms seriously rather than minimising them, create space for disclosure without judgement, share the baby’s nighttime care sufficiently to allow some sleep, and actively support access to professional help rather than waiting to see if things improve on their own.
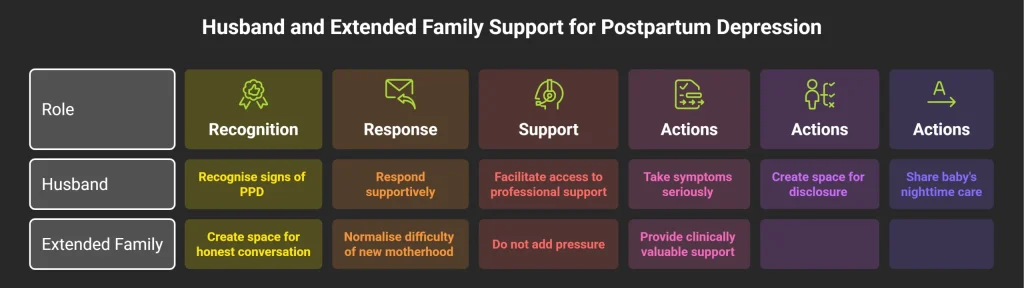
Extended family members — mothers, mothers-in-law, sisters — can also play a significant role. The family member who visits and creates space for honest conversation, who normalises the difficulty of new motherhood without making the new mother feel she is failing, and who does not add pressure through cultural expectations of performance, is providing something clinically valuable.
Evidence-Based Treatment for Postpartum Depression
Postpartum depression is highly treatable. Early identification and treatment produces faster recovery and reduces the risk of the condition becoming chronic.
Psychological Therapy
Cognitive Behavioural Therapy adapted for postpartum depression is a first-line treatment recommended by NICE. It targets the specific cognitive patterns that maintain PPD — the excessive guilt, the perfectionist standards of motherhood, the catastrophic interpretation of the baby’s crying or the difficulty of bonding — and the behavioural patterns that compound isolation and exhaustion. A meta-analysis published in The Lancet Psychiatry confirmed that psychological therapy for PPD produced significant improvement across multiple outcome measures, with effects comparable to antidepressant medication.
Interpersonal Therapy (IPT) is also specifically recommended for postpartum depression because of its focus on role transitions — the massive shift in identity, relationships, and daily structure that new parenthood represents. For Gulf-based mothers who are managing the role transition while also managing geographic isolation and cultural performance pressure, IPT’s relational and contextual focus is often particularly well-matched to the clinical picture.
Medication
For moderate to severe postpartum depression, antidepressant medication is appropriate and effective. According to NICE guidelines, SSRIs are the first-line pharmacological treatment and are considered compatible with breastfeeding, though the specific choice of medication should be discussed with a doctor who can weigh the clinical picture and the mother’s preferences. The decision about medication is a medical one, but the cultural reluctance to take antidepressants while breastfeeding — common in South Asian families — is worth addressing directly: the evidence on the safety of SSRIs in breastfeeding is well-established, and the risk of untreated severe depression to both the mother and the infant is significant.
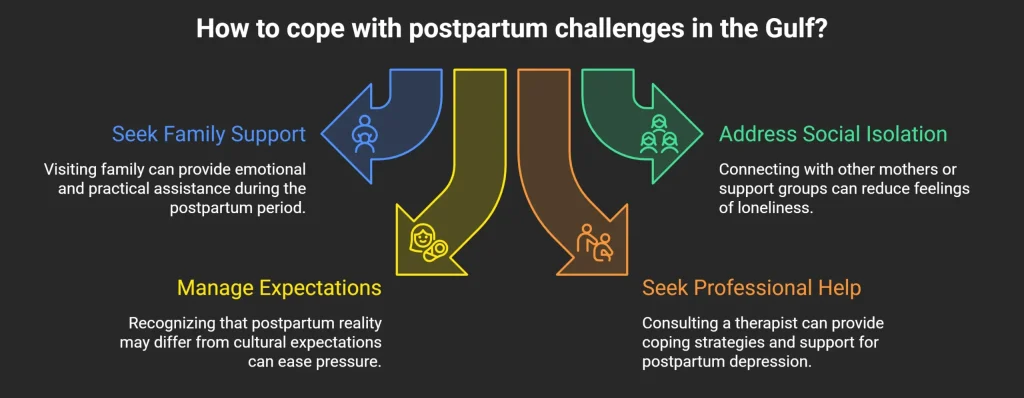
Social Support as a Clinical Intervention
The evidence on social support and PPD recovery is unambiguous: isolation worsens the condition and social connection accelerates recovery. For Gulf-based mothers, practical strategies include regular video calls with trusted people at home, connection with other South Asian mothers in the Gulf through community groups, and — where possible — arranging for extended family visits during the most acute period.
When to Seek Professional Help
Seek professional help if low mood, emotional numbness, difficulty bonding with the baby, persistent crying, or significant irritability has been present for more than two weeks after childbirth. If sleep is significantly disturbed beyond what the baby’s needs explain — lying awake when the baby sleeps, waking with dread, inability to rest even when care for the baby is available. If intrusive thoughts about harm to the baby are occurring, please speak to a professional immediately — these are a treatable symptom, not a reflection of your character, and they require proper clinical attention.
For Gulf-based mothers without easy access to a local therapist who speaks their language or understands their cultural context, online counselling in Kerala and the Gulf through Oppam offers Malayalam and Tamil-language therapy sessions via secure video call. A session can happen from home, between feeds, without creating a visible appointment or disclosing anything to the extended family before you are ready. Book your first session →
If you are based in India, the Gulf, or anywhere in the South Asian diaspora, Oppam’s therapists can work with you in Malayalam, Tamil, or English, using evidence-based approaches that are adapted to your cultural and personal context. Book your first session →
Postpartum depression is not a failure of love, faith, or character — it is a clinical condition that affects one in seven new mothers, and it responds to proper treatment. If you are a Gulf-based mother who recognises yourself in this article, you do not have to keep carrying this alone in an apartment far from everyone who knows you well. Oppam offers online counselling in Malayalam, Tamil, and English, accessible from home via secure video call, with therapists who understand both the clinical reality of PPD and the specific pressures of South Asian motherhood in the Gulf. Book your first session →
Frequently Asked Questions
What is the difference between baby blues and postpartum depression?
The baby blues affect up to 80 per cent of new mothers in the first week after birth — tearfulness, mood swings, emotional sensitivity — and resolve on their own within two weeks without treatment. Postpartum depression is a full clinical depressive episode that persists beyond two weeks, is accompanied by a broader range of symptoms including difficulty bonding, persistent low mood or emotional numbness, sleep disturbance beyond the baby’s needs, and significant functional impairment. If low mood, flatness, or distress is still present at three weeks postpartum, a clinical assessment is appropriate rather than continued waiting for it to pass.
Can postpartum depression affect fathers?
Yes. Research published in JAMA Psychiatry found that approximately 10 per cent of fathers experience postpartum depression following the birth of a child, with the highest risk in the three to six month postpartum period. Paternal PPD typically presents as irritability, withdrawal, increased work hours, alcohol use, and a sense of disconnection from the family rather than overt sadness. It is rarely recognised or treated. If a Gulf-based NRI father recognises these signs in himself following his child’s birth, the same professional support available to mothers is appropriate and accessible.
Is postpartum depression common in South Asian mothers in the Gulf?
Research on PPD in Gulf-based South Asian populations is limited but consistent with the broader literature showing that social isolation, limited support, and cultural performance pressure are significant risk factors — all of which are structurally present for many Gulf NRI mothers. The global prevalence of PPD is 10 to 15 per cent according to the World Health Organisation, and clinical experience consistently suggests this figure is an underestimate in South Asian diaspora populations where stigma and somatisation reduce disclosure and recognition. The condition is common. The silence around it is not an indication of its rarity.
Can I take antidepressants while breastfeeding?
For many SSRIs, breastfeeding is compatible with treatment, and the clinical consensus — as reflected in NICE guidelines — is that the risks of untreated severe postpartum depression to both mother and infant outweigh the risks of medication. The specific choice of antidepressant should be made with a doctor who can review the clinical picture, but the cultural assumption that medication and breastfeeding are incompatible is not supported by the current evidence. This is a conversation worth having with your doctor rather than a reason to delay treatment for severe PPD.
Can I get online therapy for postpartum depression in Malayalam or Tamil?
Yes. Oppam offers online therapy in Malayalam, Tamil, and English, accessible via secure video call from the Gulf, Kerala, or anywhere in the South Asian diaspora. For new mothers, the online format has significant practical advantages: sessions can happen at home, between feeds, without the need to arrange childcare or travel. Online therapy Kerala and Gulf through Oppam provides access to therapists trained in CBT and Interpersonal Therapy for postpartum depression, who understand the specific cultural and structural context of Gulf-based South Asian motherhood.
Will postpartum depression affect my bond with my baby long-term?
No, if it is treated. The difficulty bonding that accompanies PPD is a symptom of the depression, not evidence of a permanent relational problem. Research consistently shows that the mother-infant bond establishes fully and securely once PPD is effectively treated. The concern that feeling disconnected from the baby now means permanent damage to the relationship is itself a cognitive distortion driven by depression — and it is one that responds well to therapy. The earlier treatment is accessed, the sooner the bond that PPD is temporarily impairing can develop.
How do I tell my family I think I have postpartum depression?
This is often the hardest part. A few principles that help: choose a calm, private moment with someone you trust rather than raising it during a crisis point. Frame it in terms of how you are feeling physically as well as emotionally, “I have not been sleeping even when I can, I feel very low, I am struggling”, rather than leading with the diagnosis, which may trigger defensiveness in a family with mental health stigma. If direct conversation feels impossible initially, accessing professional support independently first gives you a clearer understanding of your own experience and, often, language and confidence for the family conversation that follows.
External Resources
-
- World Health Organisation (WHO) — Global prevalence data: anxiety disorders affect 301 million people (2022 Mental Health Atlas)
- World Health Organisation — Global prevalence of postpartum depression (10–15%); definition and clinical recognition
- The Lancet Psychiatry — Meta-analysis of psychological therapy for PPD; CBT and IPT effect sizes compared to medication
- JAMA Psychiatry — Paternal postnatal depression prevalence (approximately 10%); onset timing and presentation
- Archives of Women’s Mental Health — Social isolation as a predictor of postpartum depression; strength of association comparable to prior depression history
- NICE (UK) — Clinical guidelines for the treatment of postnatal depression; SSRI safety in breastfeeding; first-line recommendations for CBT .
- Clinical Practice & Epidemiology in Mental Health
- Khaleej Times
Struggling?
Talk to an Oppam Therapist
Get the Support You Deserve Online & Confidential