High-Functioning Depression? She has not missed a deadline in four years. Her performance reviews are excellent. She replies to messages quickly, attends every family gathering, maintains her friendships with the careful regularity of someone who knows how these things are supposed to look. If you asked anyone who knows her, they would say she is doing well. Busy, maybe. Tired, perhaps. But doing well.
She would not say that. She would say something has been wrong for a long time, though she cannot precisely identify when it started. That getting through each day requires a kind of effortful management she has never had to do before. That she feels nothing much about the things she is doing — they happen, she performs them, they do not produce the feelings they used to. That she is very good at appearing fine, and exhausted by the performance of it.
Need to Talk to Someone?
Book a private online session with a licensed therapist
This is high-functioning depression. It does not have a formal DSM diagnostic code by that name — it most commonly maps onto Persistent Depressive Disorder or a Major Depressive Episode in which the behavioural surface remains intact despite significant internal suffering. But it is real, it is clinically significant, and it is disproportionately common in South Asian communities where the cultural pressure to maintain external functioning regardless of internal state is one of the most consistent features of family and social life.
What High-Functioning Depression Is Clinically
The term “high-functioning depression” is not a formal psychiatric diagnosis. It is a useful descriptive label for presentations of depression in which the person continues to maintain significant areas of external functioning — work performance, social obligations, family responsibilities — while carrying the internal symptom burden of a depressive disorder.
The most common clinical diagnosis in this presentation is Persistent Depressive Disorder (PDD), formerly called dysthymia. PDD is characterised by a chronically depressed mood present for most of the day, on more days than not, for at least two years. The severity is typically less acute than a major depressive episode, but its duration and pervasiveness produce significant cumulative impairment. According to the American Psychiatric Association, PDD affects approximately 1.5 per cent of the global population, with a lifetime prevalence approaching 6 per cent — making it considerably more common than most people realise.
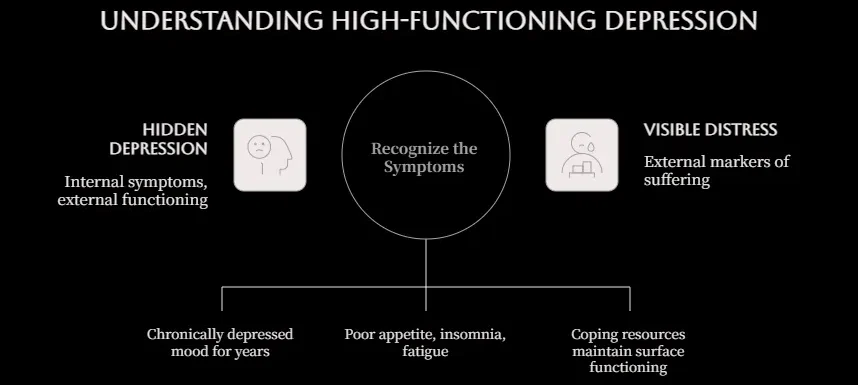
The DSM-5 requires at least two of the following additional symptoms alongside the chronically depressed mood: poor appetite or overeating, insomnia or hypersomnia, low energy or fatigue, low self-esteem, poor concentration or difficulty making decisions, and feelings of hopelessness. What is notably absent from this list is a requirement for visible distress, functional collapse, or any external marker of suffering. A person can meet full diagnostic criteria for PDD while appearing, to every external observer, to be functioning perfectly well.
High-functioning depression can also refer to a Major Depressive Episode in which the person’s coping resources, work ethic, and social skills are sufficiently developed to maintain surface functioning despite meeting the full diagnostic criteria for major depression. The maintenance of functioning in this case is not evidence of mild depression — it is evidence of the additional effort being expended to perform normality while depressed. That effort has its own cost.
Why South Asians Are Particularly Prone to This Presentation
High-functioning depression does not develop randomly. It develops in specific conditions — and many of those conditions are structural features of South Asian family and community life.
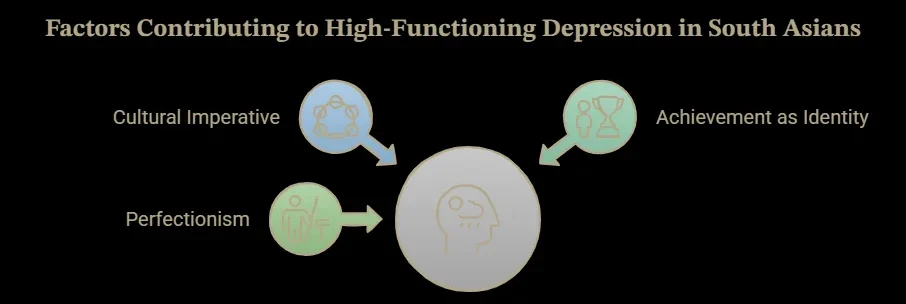
The Cultural Imperative to Continue
In Keralite families, and across South Asian communities more broadly, the expectation that an individual will manage their responsibilities regardless of how they feel is not a subtext — it is explicit. Parents who sacrificed significantly for their children’s education expect those children to succeed. Gulf NRI workers who came abroad to support the family have obligations that do not pause because they are struggling internally. Daughters-in-law who manage households while their husbands work have roles that continue regardless of their emotional state.
This imperative to continue is not malicious. It reflects a genuine set of values — commitment, endurance, family loyalty — that have real merit. But it creates the conditions for high-functioning depression because it makes stopping, disclosing, or asking for help feel like a betrayal of one’s role rather than a health decision. The person learns to function regardless of how they feel, and becomes very good at it, and the depression deepens quietly underneath a performance of capability.
Research published in Transcultural Psychiatry examining help-seeking patterns in South Asian communities found that the most commonly cited barrier to seeking mental health support was not stigma alone but a deeply internalised belief that disclosing psychological distress was incompatible with one’s responsibilities — that the people depending on you could not afford for you to not be okay. This belief is the direct cultural driver of high-functioning depression.
Achievement as Identity
Many South Asian children grow up in environments where achievement — academic, professional, financial — is the primary currency of worth. Being successful is not simply desirable; it is the condition under which love and approval feel secure. When this framework is internalised deeply, the person’s identity becomes fused with their performance. They are what they achieve.
This creates a specific vulnerability to high-functioning depression because as long as the achievements continue — as long as the performance is intact — there is no external signal that anything is wrong, and the internal suffering has no culturally intelligible language in which to be expressed. The person who is depressed but still achieving has no evidence, in their own framework, that their distress is legitimate. They keep achieving. The depression deepens.
The Specific Role of Perfectionism
Perfectionism is both a driver of high-functioning depression and one of its most consistent features. The perfectionist sets standards that cannot realistically be sustained, experiences chronic low-level failure relative to those standards, and attributes that failure to personal inadequacy rather than unrealistic expectations. The cognitive and emotional effort required to continuously reach towards an unattainable standard produces exactly the kind of chronic depletion that underlies persistent depressive disorder.
Research published in Clinical Psychology Review by Limburg and colleagues found a robust association between clinical perfectionism and both the development and the maintenance of depression, with perfectionism specifically associated with the kind of chronic, low-to-moderate severity depression characteristic of PDD rather than acute major depressive episodes. The perfectionist continues to function, continues to achieve at a high level relative to others, and continues to experience themselves as failing.
What High-Functioning Depression Feels Like From the Inside
Because high-functioning depression is so invisible externally, it is worth describing clearly what it tends to feel like from the inside — both because this may help people recognise their own experience, and because the internal picture is genuinely different from what is presented to the world.
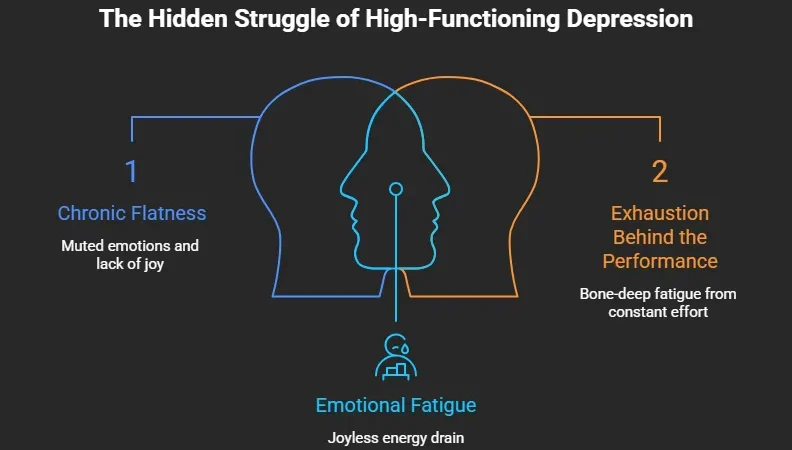
The Chronic Flatness
The most consistent feature is not sadness but a kind of emotional attenuation — everything feels muted. Positive experiences happen but do not produce the expected emotional response. A promotion, a celebration, a genuinely good conversation: these register, are processed, and produce very little feeling. The person knows they should feel something and does not. Over time this produces a secondary layer of grief about the absence of feeling, and sometimes a fear that something is fundamentally broken about their emotional capacity.
In Keralite family life, where joyful occasions — Onam, Vishu, weddings, the birth of grandchildren — are expected to be experienced with visible happiness, this flatness produces its own particular guilt. The person sits through the celebration feeling nothing and feeling guilty about feeling nothing and performing the expected happiness with increasing effort.
The Exhaustion Behind the Performance
Maintaining the external functioning of a non-depressed person while experiencing the internal state of depression requires significant energy. It involves constant self-monitoring, the suppression of visible distress, the management of interactions to prevent disclosure, and the effort of completing tasks that the depression makes harder than they should be.
According to research published in The Lancet Psychiatry on the neurological basis of depressive fatigue, the brain changes associated with depression — particularly in basal ganglia circuits involved in motivation and effort allocation — produce a genuinely increased cognitive and physical cost for voluntary actions. The person with high-functioning depression is not lazy; they are doing more work than their non-depressed counterpart for every task they complete, because the depression is adding a neurological cost to everything.
The exhaustion this produces is often described by patients as the thing they least expected: not sadness, not hopelessness, but a bone-deep tiredness that no amount of sleep resolves, and that has been present for so long they have begun to assume it is simply who they are.
The Private Hopelessness
Alongside the flatness and the exhaustion, high-functioning depression typically carries a quiet, persistent hopelessness about the future — the sense that things will not improve, that the flatness is permanent, that there is no particular reason to look forward to anything. This hopelessness is rarely expressed, because expressing it would conflict with the functioning persona. But it is present, colourising everything with a grey monotony that makes the continued effort of daily life feel increasingly pointless.
This is the aspect of high-functioning depression that carries the most clinical risk. Quiet, private hopelessness that has no outlet and no witness can progress — slowly, over months or years — into more acute suicidal ideation. The person who appears fine to everyone around them may be much further along an internal continuum of suffering than anyone knows.
How High-Functioning Depression Is Maintained
Understanding what keeps high-functioning depression going is essential for understanding what it takes to address it.
The Positive Reinforcement of Performance
One of the most counterproductive features of high-functioning depression is that the functioning is genuinely rewarded. Good performance reviews, family praise, the validation of continuing to meet obligations — these external reinforcers make it harder for the person to justify stopping. If everything appears to be working, what is the argument for change? The depression becomes the price that is paid for continued external success, and eventually this trade-off becomes normalised.
Avoidance of Inner Life
People with high-functioning depression tend to be extremely busy. The busyness is often partly strategic — keeping constantly occupied prevents the quiet that would allow the internal experience to surface. The Gulf NRI who works twelve-hour days, the Kerala housewife who is always doing something for someone else, the student who fills every spare moment with productivity: the activity is real and valuable, but it also functions as avoidance of the depression that becomes more audible when the busyness stops.
The Absence of Disclosure
Because nothing visible is wrong, there is no prompt for others to offer support, and because the cultural framework does not provide language for the internal experience, the high-functioning depressed person is typically carrying the condition completely alone. The absence of witness or acknowledgement maintains the hopelessness that nothing can change, and removes the social support that would buffer against worsening.
Evidence-Based Approaches That Actually Help
Behavioural Activation
One of the most robustly evidenced interventions for depression, including the persistent low-grade variety characteristic of high-functioning depression, is behavioural activation — the deliberate scheduling of meaningful, pleasurable, or values-aligned activities, even in the absence of motivation to pursue them.
This is clinically counterintuitive for high-functioning depressed people because they are already doing many activities. The distinction is between activities performed out of obligation and activities chosen for their own sake — for genuine enjoyment, meaning, or personal value. High-functioning depression typically involves a life full of the former and empty of the latter. Behavioural activation for this population is less about doing more and more about doing differently: introducing activities that exist for the person rather than for their roles.
Cognitive Work on Perfectionism and Self-Worth
CBT adapted for persistent depression addresses the specific cognitive patterns that drive it — particularly the perfectionist standards that make chronic low-level failure feel like evidence of fundamental inadequacy. Examining the evidence for these standards, testing them against realistic comparison points, and developing a more accurate and compassionate self-assessment is central to the cognitive work.
According to a meta-analysis published in Psychological Medicine, CBT for persistent depressive disorder produces significant improvements in depressive symptoms and is superior to usual care at follow-up. The cognitive component — addressing the specific beliefs about self-worth and achievement that drive the depression — is particularly important for the high-functioning presentation because these beliefs are often so deeply internalised they are experienced as facts rather than thoughts.
Addressing the Mask
A specific therapeutic goal in high-functioning depression is the gradual dismantling of the performance — not collapsing functioning, but creating spaces in which the internal experience can be expressed rather than suppressed. For South Asian patients, this often begins in the therapy room itself, which is frequently the first context in which the honest internal experience has been voiced at all. The relief of being witnessed, of having the experience named and taken seriously, is itself clinically significant.
When to Seek Professional Help
High-functioning depression specifically warrants professional support because it is the presentation least likely to self-refer. The external functioning provides apparent evidence that things are manageable. The internal suffering provides the hopelessness that change is possible. The cultural framework provides the expectation that endurance is the appropriate response. All three forces point away from help-seeking.
Seek professional support if the emotional flatness has been present most days for six months or more. If the effort of maintaining daily functioning feels significantly greater than it should, and has for an extended period. If there is a persistent private hopelessness about the future that you would not disclose to anyone. If pleasurable activities — those chosen for their own sake rather than out of obligation — have become entirely absent from your life. If the exhaustion is chronic and unrelieved.
For Keralites in Kerala and the diaspora, online counselling in Kerala through Oppam offers access to therapists who work in Malayalam, Tamil, and English and understand the specific cultural dynamics that produce and maintain high-functioning depression in South Asian life. The online format means you do not need to create a visible appointment or disclose anything to anyone before you are ready. Book your first session →
High-functioning depression is real, it is clinically significant, and it does not get better by continuing to function through it — it deepens. If you have been carrying a private exhaustion, flatness, or hopelessness that your external life gives no evidence of, that gap between how you appear and how you feel is worth taking seriously. Oppam offers online counselling in Kerala and across the South Asian diaspora in Malayalam, Tamil, and English, with therapists who understand both the clinical reality of this presentation and the cultural dynamics that keep it hidden for so long. You do not have to be visibly unwell to deserve proper support. Online Counselling in Kerala →
Frequently Asked Questions
What is high-functioning depression?
High-functioning depression refers to presentations of depression in which the person continues to maintain significant external functioning — meeting work responsibilities, managing family obligations, maintaining social relationships — while carrying the internal burden of a depressive disorder. It most commonly maps clinically onto Persistent Depressive Disorder, a condition involving chronically low mood present on most days for two years or more. The functional surface is not evidence of mild depression; in many cases it reflects the additional effort being expended to perform normality while genuinely suffering internally.
Can you be depressed if you are still functioning normally?
Yes, completely. The clinical criteria for depression and Persistent Depressive Disorder do not require visible functional collapse. They require the internal symptom burden — persistent low mood, loss of pleasure, fatigue, hopelessness — to be present and causing distress. Many people with clinical depression maintain significant external functioning through effort, coping mechanisms, and cultural or personal obligation. The functioning does not indicate that the depression is mild or does not require treatment. In high-functioning presentations, it often indicates the opposite — that the person is working exceptionally hard to maintain a surface that does not reflect their internal state.
Why is high-functioning depression so common in South Asian families?
Several converging cultural factors make this presentation particularly prevalent in South Asian communities. The imperative to continue functioning regardless of internal state — driven by family obligation, financial responsibility, and the cultural valorisation of endurance — actively suppresses the disclosure and recognition of depression. Achievement-based self-worth means that as long as performance is maintained, there is no culturally intelligible evidence of suffering. And the limited vocabulary for psychological distress in many South Asian languages and family cultures makes the experience difficult to name even privately. These are structural features of the culture, not individual failings.
How long can high-functioning depression go unnoticed?
A very long time. Persistent Depressive Disorder, the most common clinical presentation underlying high-functioning depression, requires symptoms to have been present for two years to meet diagnostic criteria — and in practice, many people present to clinical services having carried the condition for five, ten, or fifteen years. In South Asian contexts, where the cultural framework provides explanations other than depression (stress, tiredness, personality, life circumstances), and where help-seeking carries significant stigma, the gap between onset and first treatment can be extremely long. This is one of the strongest arguments for early recognition and assessment.
Where can I find online therapy in Kerala for depression?
Oppam offers access to online psychologists in Kerala and across the South Asian diaspora, in Malayalam, Tamil, and English. Sessions are conducted via secure video call and are accessible without a GP referral or clinic visit. Online therapy Kerala through Oppam is particularly appropriate for high-functioning depression, where the privacy of online delivery removes the social visibility of help-seeking that many South Asians cite as a primary barrier to accessing care.
Is high-functioning depression less serious than other depression?
No. Despite the maintained external functioning, high-functioning depression involves genuine clinical-level suffering and carries significant risks if left untreated, including progression to more acute depressive episodes, development of comorbid anxiety disorders, increased alcohol use, and in some cases, suicidal ideation that remains private precisely because the external functioning provides no visible signal of distress. The functioning obscures the severity rather than reducing it. Persistent Depressive Disorder that goes untreated for years produces real and lasting effects on quality of life, relationships, and health that warrant the same clinical attention as any other depressive presentation.
Can high-functioning depression be treated without taking time off work?
Yes, for most presentations. Therapy for persistent depression and high-functioning depression typically does not require any disruption to work or social functioning. CBT and other evidence-based approaches are delivered in weekly sessions of fifty to sixty minutes, and the cognitive and behavioural changes occur gradually without requiring a visible change in the person’s external life. For many South Asian patients, the fact that treatment does not require disclosure, leave from work, or any visible departure from their normal functioning is the factor that makes accessing it finally possible.
External Resources
-
- World Health Organisation (WHO) — Global prevalence data: anxiety disorders affect 301 million people (2022 Mental Health Atlas)
- World Health Organisation — Global prevalence of postpartum depression (10–15%); definition and clinical recognition
- The Lancet Psychiatry — Meta-analysis of psychological therapy for PPD; CBT and IPT effect sizes compared to medication
- JAMA Psychiatry — Paternal postnatal depression prevalence (approximately 10%); onset timing and presentation
- Archives of Women’s Mental Health — Social isolation as a predictor of postpartum depression; strength of association comparable to prior depression history
- NICE (UK) — Clinical guidelines for the treatment of postnatal depression; SSRI safety in breastfeeding; first-line recommendations for CBT .
- Clinical Practice & Epidemiology in Mental Health
- Khaleej Times
- American Psychiatric Association / DSM-5 — Diagnostic criteria for Persistent Depressive Disorder; prevalence data (1.5% current, 6% lifetime)
- Psychological Medicine — Meta-analysis of CBT for persistent depressive disorder; superiority over usual care at follow-up
- Clinical Psychology Review (Limburg et al.) — Association between clinical perfectionism and persistent low-to-moderate severity depression; mechanism of maintenance
- Amaha – What is High Functioning Depression and Anxiety? An Indian Perspective.
Struggling?
Talk to an Oppam Therapist
Get the Support You Deserve Online & Confidential