depression symptoms causes treatment ?It does not always look like crying. Sometimes it looks like a person who gets up every morning, goes to work, manages their responsibilities, and feels absolutely nothing. Not sadness exactly — more like a flat, colourless version of a life that used to have texture. Food tastes different. Sleep comes but does not restore. The things that once brought genuine pleasure — a phone call with a close friend, a meal, a film — now require effort to initiate and produce little when they happen.
This pattern is familiar to more people than admit it. In South Asian families — particularly Keralite households where health is a subject of constant communal attention, where elderly relatives narrate their symptoms in detail at every gathering, and where a missed doctor’s visit feels irresponsible — concern about health is culturally embedded and often indistinguishable from care. The mother who worries about every headache, the father who reads medical articles at midnight, the NRI professional who arranges annual health checks with anxious precision: these figures are not unusual. What is less visible is when that concern tips into something that causes genuine psychological suffering, regardless of whether any physical illness is ever found.
Need to Talk to Someone?
Book a private online session with a licensed therapist
Health anxiety, formerly labelled hypochondria, is a recognised clinical condition. It involves persistent, excessive preoccupation with the belief that you have, or are developing, a serious illness, despite medical reassurance to the contrary. It is not about being dramatic or weak-willed. It is a specific anxiety pattern with identifiable cognitive and behavioural drivers, and it responds to treatment.
What health anxiety is, why it is particularly common in South Asian communities, how to distinguish it from legitimate medical concern, and what actually helps…. Read more
What Is Health Anxiety?
Health anxiety, now formally classified as Illness Anxiety Disorder in the DSM-5, is characterised by excessive and disproportionate worry about having or acquiring a serious illness. The person may have minimal or no physical symptoms, or they may have symptoms that are real but are interpreted in a catastrophic way that far exceeds what the medical evidence supports.
The older term “hypochondria” or “hypochondriasis” carried unfortunate connotations of fabrication or attention-seeking that were never clinically accurate. The current terminology reflects a better understanding: health anxiety is an anxiety disorder, not a personality flaw or a failure of character. The suffering it produces is real, even when the illness it fears is not.
It is worth noting that the DSM-5 also retains a related category called Somatic Symptom Disorder, which applies when the person does have significant physical symptoms but their distress and preoccupation about those symptoms are disproportionate. Health anxiety and somatic symptom disorder overlap considerably in clinical practice, and both involve the same core pattern of excessive health-focused worry.
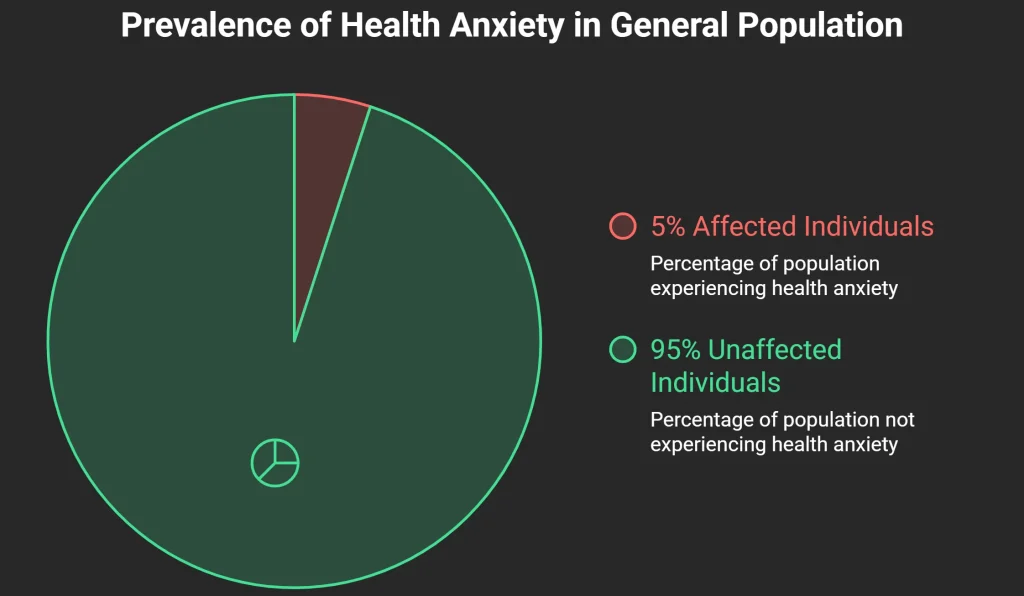
According to research published in the Journal of General Internal Medicine, health anxiety affects between 4 and 6 per cent of the general population. In primary care settings, where patients present with medically unexplained symptoms, the prevalence is considerably higher. The condition cuts across cultures and demographics, but the form it takes — which illnesses are feared, how symptoms are communicated, how medical help is sought and used — is shaped significantly by cultural context.
psychologist’s voice: “Absolutely — and please do. A friend who listens without judgement is one of the most underrated things a person can have. But talking to a friend and seeing a psychologist are solving two different problems. Your friend can make you feel less alone. A psychologist can make you less anxious. Both matter. Neither replaces the other.“
Why South Asians Are Particularly Vulnerable
Health anxiety does not develop in isolation from culture, and in South Asian communities there are several converging factors that make it both more likely and harder to identify.
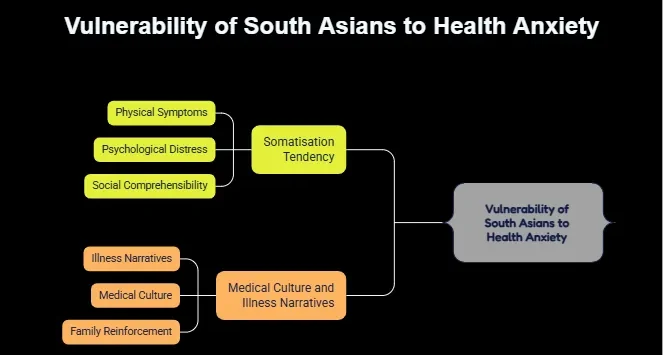
The Somatisation Tendency
Across South Asian clinical populations, there is a well-documented pattern of somatisation: the expression of psychological distress through physical symptoms and a tendency to seek physical rather than psychological explanations for suffering. Research published in the Indian Journal of Psychiatry has consistently described this pattern in both urban and rural populations, noting that patients often present to general physicians and specialists repeatedly before a psychological cause is explored.
This does not mean South Asians are more neurotic or more physically fragile. It reflects the fact that in many South Asian families, emotional distress does not have a well-developed vocabulary or a sanctioned means of expression. Saying “I am anxious” or “I am struggling psychologically” may feel too vulnerable, too abstract, or too stigmatised. Saying “my chest hurts” or “I have not been well” is socially comprehensible and does not carry the same shame. The body becomes the available channel for communicating what the mind is holding.
In this context, health anxiety can look like diligent self-care — and it is treated that way by families, who may reinforce the pattern by accompanying the person to every appointment and treating each new symptom with grave concern.
Medical Culture and Illness Narratives
In Kerala specifically, where literacy rates and health awareness are among the highest in India, there is also a particular cultural comfort with medical knowledge. Families discuss diagnoses, track symptoms, and follow treatment plans with a level of engagement that would be unusual elsewhere. This is, in many respects, a public health asset. But it also creates a context where health monitoring can tip into health hypervigilance — where the line between staying informed and becoming consumed by the fear of illness is easy to cross.
The Gulf diaspora adds another layer: far from family networks and familiar healthcare systems, NRIs often carry the weight of managing their health alone, in countries where private healthcare is expensive and the social safety net is different from home. A symptom that at home would be discussed with a parent, a sibling, or a trusted family doctor becomes a private preoccupation, processed with Google Search as the only available consultant.
How Health Anxiety Thinks: The Cognitive Patterns
Understanding how health anxiety operates cognitively is essential both for recognising it and for treating it.
Probability Overestimation
People with health anxiety systematically overestimate the likelihood that their symptoms indicate serious illness. A headache is not stress or dehydration — it is a potential tumour. A brief heart flutter is not caffeine — it is arrhythmia. This is not a conscious choice. It is a habitual cognitive pattern, often operating below the level of deliberate thought, that assigns very high probability to worst-case outcomes.
Catastrophic Interpretation
Related but distinct, catastrophic interpretation involves not just overestimating the likelihood of illness but also assuming the most severe version of any potential diagnosis. The possibility that the chest tightness is musculoskeletal is dismissed; only the cardiac explanation carries emotional weight.
Safety-Seeking Behaviours
What keeps health anxiety maintained is not the medical investigations — it is what happens around them. According to the cognitive model of health anxiety developed by Paul Salkovskis and colleagues at Oxford University, and validated in multiple clinical trials, safety-seeking behaviours are the primary maintenance mechanism. These include:
- Repeated googling of symptoms
- Seeking reassurance from family members, GPs, or multiple specialists
- Checking the body for symptoms (palpating lymph nodes, monitoring heart rate, examining skin)
- Avoiding medical news, health articles, or conversations about illness (paradoxically reinforcing the sense that the topic is dangerous)
Each safety-seeking behaviour provides temporary relief but prevents the anxiety from naturally habituating. The person never learns, at an experiential level, that the feared illness is not present — because the checking behaviour interrupts that learning before it can consolidate.
Distinguishing Health Anxiety from Legitimate Medical Concern
This is the question people with health anxiety ask most frequently, and it deserves a careful answer.
Legitimate medical concern involves proportionate attention to a real symptom over a reasonable period of time, followed by appropriate medical consultation and the ability to accept reassurance when investigations are normal. The concern has a beginning and an end.
Health anxiety is distinguished by several features. The worry persists after negative investigations — the person feels relieved briefly, then finds a new symptom or decides the tests might have missed something. The worry is pervasive, occupying significant mental bandwidth across the day. Multiple doctors have been consulted for the same concern, sometimes across specialties. The person avoids medical news or health conversations not because they are uninterested but because exposure intensifies anxiety rather than providing information. And crucially, the preoccupation causes distress and functional impairment in its own right — not just the physical symptom, but the worry about it.

It is also worth naming what health anxiety is not. It is not the same as being diligent about health. Regular screenings, attending to new or unusual symptoms, maintaining medical follow-up for known conditions — all of these are appropriate health behaviours. The distinction lies in proportion, duration, and the capacity to accept reassurance.
What Actually Helps: Evidence-Based Treatment
Cognitive Behavioural Therapy
Cognitive Behavioural Therapy is the most strongly evidenced treatment for health anxiety. A landmark randomised controlled trial published in The Lancet by Clark, Salkovskis, and colleagues demonstrated that CBT for health anxiety produced significantly greater improvements than standard medical care, with benefits maintained at 12-month follow-up.
CBT for health anxiety works on both the cognitive and behavioural dimensions of the condition. On the cognitive side, it helps the person identify and examine their specific interpretations — when they notice a symptom and assume the worst, the work involves asking: what is the realistic probability here, and am I considering all explanations proportionately? On the behavioural side, it involves a structured reduction in safety-seeking behaviours, with gradual exposure to health-related triggers, so that anxiety naturally habituates rather than being perpetually maintained by checking and reassurance.
A practical starting point is a symptom diary kept not to monitor symptoms medically, but to track the relationship between anxiety levels, life stressors, and symptom intensity. Many people are surprised to discover that their worst symptom days correlate closely with periods of stress or poor sleep — evidence that the anxiety system, not a disease process, is generating much of what they feel.
Reducing Reassurance-Seeking
One of the most clinically challenging aspects of treating health anxiety is the role of the family. In South Asian households, family members are typically deeply involved in health management. When a person with health anxiety seeks reassurance from a family member — “Do you think this could be serious?” “Should I go back to the doctor?” — the reassurance provided, however well-intentioned, feeds the cycle rather than breaking it.
Effective treatment involves working not just with the individual but with the patterns in their relationships. Family members who understand why reassurance is counterproductive can be significant allies in recovery.
Acceptance and Commitment Therapy
Acceptance and Commitment Therapy offers a complementary approach that is particularly useful when the goal of eliminating health anxiety feels overwhelming. Rather than directly challenging anxious thoughts, ACT works on increasing psychological flexibility — the ability to hold anxious thoughts without being controlled by them, and to take meaningful action in line with values even when anxiety is present. For health anxiety, this often involves the recognition that some uncertainty about health is unavoidable, and that attempting to achieve certainty through checking and reassurance-seeking is itself the source of the suffering.
When to Seek Professional Help
Health anxiety warrants professional support when it is occupying a significant portion of your mental life on most days. If you have had repeated medical investigations for the same concern and the normal results have not reassured you, that gap between what the medicine says and what you believe is clinically meaningful. If you are spending more than an hour a day thinking about your health, researching symptoms, or seeking reassurance, the anxiety itself is the problem that needs addressing.
If family relationships are being affected — if a partner or parent has become a primary reassurance source and this is creating tension, or if the health anxiety is driving conflict about medical consultations — that is a further indicator that structured support is needed.
If you are based in Kerala and looking for professional support, online counselling in Kerala through Oppam means you do not have to wait for a clinic appointment or manage the privacy concerns that can arise from attending mental health services in person in a community where everyone knows each other. Oppam’s therapists are trained in CBT and other evidence-based approaches for health anxiety, and work in Malayalam, Tamil, and English.
If you are based in India, the Gulf, or anywhere in the South Asian diaspora, Oppam’s therapists can work with you in Malayalam, Tamil, or English, using evidence-based approaches that are adapted to your cultural and personal context. Book your first session →
Frequently Asked Questions
What is health anxiety and how do I know if I have it?
Health anxiety involves persistent, excessive worry about having or developing a serious illness, despite medical reassurance to the contrary. You may recognise it by a pattern of repeated symptom-checking, frequent medical consultations for the same concern, an inability to feel genuinely reassured by normal test results, and significant daily preoccupation with your health. The key marker is that the worry itself is causing distress and interfering with your daily life, regardless of whether any physical illness is found. If this pattern has been present for six months or more, a clinical assessment is appropriate.
Is health anxiety the same as being a hypochondriac?
“Hypochondria” was the older clinical term, now largely replaced by Illness Anxiety Disorder in the DSM-5. The older term carried inaccurate connotations of fabrication or attention-seeking. Health anxiety is a genuine anxiety disorder with identifiable cognitive and behavioural mechanisms — not a personality type or a failure of character. The suffering it produces is real, the patterns that maintain it are well understood, and it responds to evidence-based treatment. Using the updated terminology reflects a more accurate and compassionate understanding of the condition.
Can googling symptoms make health anxiety worse?
Yes, and this is one of the most reliably identified maintenance factors for health anxiety. Searching symptoms online almost always produces worst-case results — cancer, rare diseases, serious conditions — because medical literature describes the full range of diagnostic possibilities, not the base rates. For someone without health anxiety, this is manageable. For someone with health anxiety, it provides brief reassurance followed by new fears and further searching. Reducing or stopping symptom googling is typically one of the first behavioural targets in CBT for health anxiety, and many people notice significant improvement within weeks of stopping.
Why is health anxiety so common in South Asian families?
Several cultural factors converge. There is a well-documented tendency in South Asian populations to express psychological distress physically rather than emotionally, which means anxiety often presents as physical symptoms rather than reported worry. In communities where illness carries significant family concern and medical help-seeking is strongly supported, health vigilance is culturally reinforced. In Gulf and diaspora settings, social isolation and distance from familiar healthcare can intensify the pattern. And significant stigma around mental health diagnoses means the anxiety component often goes unrecognised while the physical symptom presentation receives all the attention.
Where can I find an online psychologist consultation in Kerala for health anxiety?
Oppam offers online psychologist consultations for clients in Kerala and across the South Asian diaspora, in Malayalam, Tamil, and English. Sessions are conducted via secure video call and are accessible from anywhere with an internet connection. This removes the practical and social barriers of in-person attendance and allows for consistent, structured treatment regardless of your location. Oppam’s Online therapists are trained in CBT for health anxiety and can work with you on both the cognitive patterns and the safety-seeking behaviours that maintain the condition.
Can health anxiety cause real physical symptoms?
Yes, and this is one of the most important things to understand. Anxiety activates the body’s stress response, which produces genuine physiological effects: muscle tension, headaches, digestive disturbance, palpitations, fatigue, tingling, and dizziness. These symptoms are real and measurable. In health anxiety, they are then misinterpreted as evidence of serious illness, which increases anxiety, which intensifies the symptoms — a self-reinforcing cycle. This is why many people with health anxiety do experience real physical symptoms; the question is their cause. Understanding that anxiety itself generates physical sensations is often the beginning of meaningful change.
Can health anxiety be treated without medication?
Yes. Psychological therapy, particularly CBT, is the first-line and most durable treatment for health anxiety according to NICE guidelines. Medication — typically SSRIs — may be recommended alongside therapy for moderate to severe cases, or when the anxiety is significantly impairing function. But therapy alone produces substantial improvement for the majority of people with health anxiety, and the cognitive and behavioural skills developed in therapy provide tools that persist after treatment ends. Medication alone, without addressing the underlying cognitive patterns, tends to provide only temporary relief.
External Resources
-
- World Health Organisation (WHO) — Global prevalence data: anxiety disorders affect 301 million people (2022 Mental Health Atlas)
- American Psychiatric Association / DSM-5 — Diagnostic criteria for GAD, panic disorder, social anxiety disorder
- JAMA Psychiatry — Meta-analysis of CBT efficacy for anxiety disorders; equivalence of online and in-person delivery
- International Journal of Social Psychiatry — Acculturation stress and elevated anxiety/depression rates in South Asian diaspora populations in the UK
- Indian Journal of Psychiatry — Somatisation of psychological distress in Indian clinical populations
- NICE (UK) — Clinical guidelines for the treatment of GAD; first-line recommendations for SSRI/SNRI use
- Transcultural Psychiatry — Acculturation stress and elevated GAD rates in South Asian migrant populations
- NHS
Struggling?
Talk to an Oppam Therapist
Get the Support You Deserve Online & Confidential