Exam Anxiety in Kerala Students increasing day by day.! The SSLC results are three weeks away. A seventeen-year-old in Thrissur has not slept properly in ten days. She knows the material — she has studied it, revised it, written practice answers until her hand ached. But when she sits at her desk now, her mind goes blank. Her heart races for no reason she can identify. She snaps at her mother, cries without warning, and lies awake at midnight convinced she has forgotten everything she ever learned.
Her parents tell her to stop worrying and study harder. Her teachers tell her the exam is not the end of the world, then in the next breath remind the class that these marks will follow them forever. She is not sure which message to believe. What she knows is that something does not feel right, and she does not have the words for it.
Need to Talk to Someone?
Book a private online session with a licensed therapist
This is exam anxiety — not nervousness, not laziness, not a lack of discipline. It is a specific psychological response that is extremely common among students in Kerala, where academic performance carries intense personal, familial, and social weight. It is also, when it reaches a certain level, genuinely impairing: it makes the very thing you are trying to do harder to do.
What Exam Anxiety Actually Is
Exam anxiety is a form of performance anxiety — a psychological state in which the evaluation context itself triggers a fear response that interferes with cognitive functioning. It is not the same as simply feeling nervous before an important test, which is normal and, in moderate doses, useful. It is the experience of anxiety so intense that it disrupts concentration, memory retrieval, and decision-making at precisely the moment they are most needed.
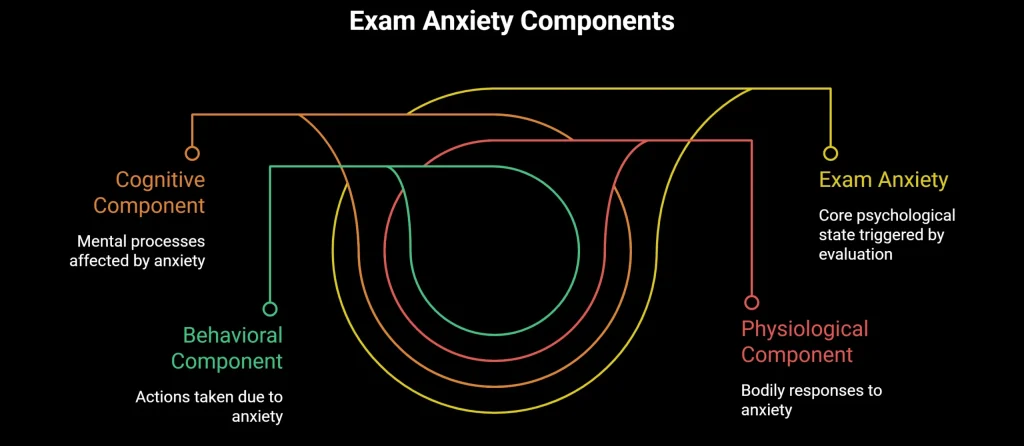
Clinically,exam anxiety involves three interconnected components. The cognitive component includes intrusive worried thoughts, difficulty concentrating, mental blanking, and catastrophic predictions about outcomes. The physiological component includes increased heart rate, sweating, nausea, headaches, and disturbed sleep. The behavioural component includes avoidance of study material, procrastination driven by dread rather than laziness, and reassurance-seeking from family members.
According to research published in the International Journal of Environmental Research and Public Health, exam anxiety affects between 25 and 40 per cent of students globally, with higher rates in academic environments characterised by high-stakes testing and significant social pressure around results. India consistently falls into this high-pressure category, and Kerala, with its historically strong emphasis on educational achievement as a pathway to economic and social mobility, produces particularly acute versions of this pattern.
The Yerkes-Dodson law, a well-established principle in psychology, describes an inverted U-shaped relationship between arousal and performance: some level of stress improves performance by sharpening focus, but beyond an optimal point, further arousal degrades it. Exam anxiety pushes students past that optimal point, which is why the student who panics during an exam often performs below their actual level of preparation.
Why Kerala Students Face Particular Pressure
To understand exam anxiety in Kerala, you have to understand what exams mean in Kerala — and that meaning is not primarily academic.
The Weight of Family Investment
In most Keralite families, a child’s education is not a private matter. It is a collective project. Parents sacrifice significantly — financially, socially, in terms of their own time and energy — for their children’s academic success. Grandparents reference it. Relatives enquire about it at every family gathering. The results of the SSLC, the Plus Two, the NEET, the entrance exams are not just the student’s results. They are the family’s results, discussed at the level of the neighbourhood and the church or mosque community.
This collective investment is rooted in genuine love and real economic logic — education has been the primary route out of financial precarity for generations of Keralite families, and that history is not imaginary. But it creates a psychological burden for the student that extends far beyond their own aspirations. Failing an exam does not feel like a personal setback. It feels like a betrayal of everyone who has invested in you.
Comparison Culture
Kerala’s high literacy rates and dense social networks create a specific comparison environment. Students are acutely aware of how their peers are performing — through tuition centres, WhatsApp groups, relatives who helpfully share other children’s marks, and a cultural comfort with direct questions about results that would be considered intrusive in many other settings. This constant social comparison amplifies individual anxiety by adding the dimension of public performance to an already high-stakes private one.
The NEET and Entrance Exam System
For students aiming at medicine or engineering, the entrance exam system adds another layer of pressure that is qualitatively different from school examinations. The NEET, in particular, has generated significant psychological distress across Kerala and Tamil Nadu since its national implementation. The combination of a single high-stakes test, fierce competition, the collapse of alternative pathways for many families, and years of preparation compressed into one sitting creates anxiety conditions that are clinically distinct from ordinary exam stress. Research from NIMHANS has documented the mental health impact of entrance exam pressure on Indian students, including elevated rates of depression, anxiety disorders, and in the most severe cases, suicidal ideation.
How Exam Anxiety Affects the Brain
Understanding the neuroscience of exam anxiety is practically useful because it explains why certain strategies work and others do not.
When the brain perceives a threat — and a high-stakes exam, in a context of intense social pressure, registers as a genuine threat to a student’s nervous system — the amygdala activates the fight-or-flight response. Cortisol and adrenaline flood the system. The prefrontal cortex, which handles working memory, complex reasoning, and retrieval of stored information, is effectively suppressed in favour of survival-oriented responses.
This is why students who have studied thoroughly find themselves unable to recall information during the exam. The knowledge is there. The physiological state of acute anxiety is temporarily blocking access to it. This is not a character failing. It is a neurological event.
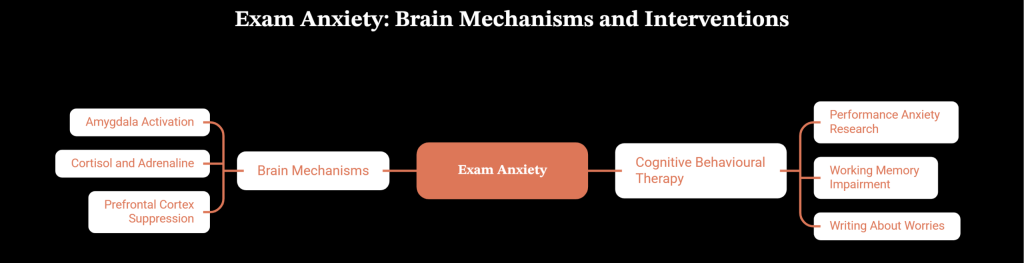
Cognitive Behavioural Therapy research on performance anxiety, including work by Dr Sian Beilock at the University of Chicago published in Science, has confirmed that high-pressure testing situations specifically impair working memory in students with high anxiety — and that targeted psychological interventions can restore that capacity. One of Beilock’s most cited findings is that simply writing about your worries for ten minutes before an exam can measurably improve performance by offloading the cognitive burden of anxious rumination.
What Actually Helps: Evidence-Based Strategies
Expressive Writing Before Exams
As noted above, research published in Science by Beilock and colleagues demonstrated that students who spent ten minutes writing freely about their exam worries immediately before a test performed significantly better than those who did not. The effect was most pronounced for students with the highest levels of test anxiety.
This is not journalling as a general wellness practice. It is a specific pre-exam technique: sit down ten minutes before the paper begins, write freely and uncensored about everything you are worried about, then put the paper away. The mechanism appears to be the externalisation of anxious content from working memory, freeing up cognitive capacity for the task itself. It is practical, costs nothing, and has direct experimental support.
Separating Performance from Identity
Much of the cognitive work in treating exam anxiety involves helping students disentangle their performance in a test from their sense of personal worth. This sounds obvious when stated directly; it is psychologically very difficult to achieve in a cultural context where these two things have been systematically linked throughout childhood.
A CBT technique that is useful here is cognitive restructuring of the specific thought patterns that drive exam anxiety. The most common pattern is catastrophic thinking: “If I fail this exam, my life is over / my parents will be devastated / I will never recover.” Examining these thoughts involves asking: Is this literally true? What would actually happen? Have I recovered from setbacks before? What does the evidence suggest about my resilience?
This is not toxic positivity or the instruction to simply think happy thoughts. It is a structured examination of whether the catastrophic thought is an accurate prediction or an anxiety-driven distortion.
Sleep as a Non-Negotiable
One of the most counterproductive patterns in Kerala student culture during exam season is the sacrifice of sleep for study time. Late-night and all-night study sessions are treated as evidence of dedication. Clinically, they are counterproductive. According to research from the Division of Sleep Medicine at Harvard Medical School, sleep plays a critical role in memory consolidation — the process by which newly learned material is transferred from short-term to long-term memory. Studying without sleeping is the cognitive equivalent of filling a container with a hole in it.
Students who sleep seven to nine hours during exam preparation retain more, retrieve more accurately, and regulate their emotional responses better during the exam itself. Framing sleep as a study tool rather than a luxury is both clinically accurate and sometimes more persuasive in a culture that equates rest with laziness.
Structured Study and the Reduction of Avoidance
Exam anxiety frequently drives avoidance — the student feels so overwhelmed by the material that they cannot begin, so they do something else, feel guilty, feel more anxious, and avoid further. This cycle is broken not by willpower but by structure.
Behavioural activation principles from CBT suggest breaking study tasks into the smallest possible units and scheduling them across the day with built-in breaks. The goal is not to study harder but to reduce the aversiveness of starting, which is where the avoidance takes hold. A student who commits to ten minutes on one chapter is more likely to continue than one who sits down intending to cover the entire syllabus.
What Parents Can Do (and Stop Doing)
This section is for parents, because in Kerala, exam anxiety is rarely a student problem alone.
The most common parental contribution to exam anxiety is the expression of anxiety about the exam while instructing the student not to be anxious. “Don’t worry, just study” is not reassuring when it is delivered by a parent who is visibly worried. Children are acutely sensitive to parental emotional states, and the message received is often “this is very serious and frightening” rather than “this is manageable.”
What actually helps is creating an environment where the student’s effort is acknowledged separately from their results, where failure is discussed as something survivable rather than catastrophic, and where the parent’s own anxiety is managed away from the student rather than expressed in their presence.
This is genuinely difficult for parents who are themselves anxious about outcomes they cannot control. It may be worth acknowledging that parental anxiety about children’s exams is real, valid, and also in need of management — not suppression, but somewhere other than in the student’s study space.
When to Seek Professional Help
Exam-related stress that resolves after results, or that responds to the strategies above, is within the normal range. The following signs indicate that professional support is warranted.
If anxiety is preventing sleep for more than a few consecutive nights, that sleep debt alone requires attention. If the student is experiencing panic attacks — sudden episodes of racing heart, chest tightness, difficulty breathing, or a sense of losing control — during or outside of study periods, that is a clinical symptom that warrants assessment. If the student is avoiding school, refusing to attend exams, or showing signs of significant mood change (withdrawal, persistent sadness, loss of interest in everything, not just studies), those are indicators that the anxiety has moved beyond exam stress into something more pervasive.
For exam anxiety that is impairing functioning but has not reached crisis level, structured psychological support works. Oppam offers online counselling for students and families in Malayalam, Tamil, and English, with therapists trained in CBT for performance anxiety. Sessions are accessible from home, which removes the barrier of attending a clinic during an already pressured period.
If you are based in India, the Gulf, or anywhere in the South Asian diaspora, Oppam’s therapists can work with you in Malayalam, Tamil, or English, using evidence-based approaches that are adapted to your cultural and personal context. Book your first session →
Frequently Asked Questions
What are the signs of exam anxiety in students?
Exam anxiety goes beyond pre-exam nervousness. Signs include persistent difficulty sleeping in the weeks before exams, physical symptoms such as headaches, nausea, or stomach problems that worsen around study or exam periods, difficulty concentrating on material the student has already covered, tearfulness or irritability disproportionate to the situation, and a pattern of avoidance where the student struggles to begin studying despite wanting to. If these symptoms are present consistently rather than just on exam day, and if they are impairing daily functioning, a clinical assessment is appropriate.
Is exam anxiety normal for Kerala students?
A degree of performance anxiety before high-stakes exams is normal and even useful — it sharpens attention and motivates preparation. What is not inevitable is anxiety so intense that it disrupts sleep, blocks memory retrieval during exams, or causes the student to perform significantly below their actual level of preparation. Kerala’s educational culture creates specific pressures that amplify this anxiety beyond the normal range for many students, which is why targeted support is both appropriate and effective.
How can I help my child with exam anxiety?
The most important thing is to separate your child’s worth from their results — explicitly and repeatedly. Acknowledge their effort rather than predicting or demanding outcomes. Avoid expressing your own anxiety about results in front of them. Ensure they are sleeping adequately, eating regularly, and taking real breaks. If the anxiety is severe — disrupting sleep, causing physical symptoms, or leading to avoidance of study altogether — professional support is appropriate and need not wait until after the exam season.
Can exam anxiety affect NEET or entrance exam performance?
Yes, significantly. NEET preparation involves years of high-intensity study followed by a single high-stakes sitting, which is a near-perfect formula for performance anxiety. Research from NIMHANS has documented elevated rates of anxiety and depression among NEET aspirants in India. The cognitive effects of acute anxiety — working memory impairment, difficulty with retrieval, catastrophic thinking during the paper — can cause students to underperform relative to their genuine preparation level. Structured psychological support before entrance exams is not a luxury; for students with significant anxiety, it is a practical performance intervention.
Can online therapy help with exam anxiety?
Yes. CBT delivered online has been shown in multiple studies to be as effective as face-to-face therapy for anxiety, including performance anxiety. For students, online therapy has the additional advantage of fitting around study schedules, removing the time cost of travel, and maintaining privacy — a student does not need to explain to their tuition centre why they are visiting a psychologist. Oppam offers online sessions in Malayalam, Tamil, and English, which means a student can work with a therapist in their first language without needing to translate their experience.
My parents keep comparing me to other students. How do I handle this?
This is one of the most common contributors to exam anxiety in Kerala, and it is genuinely difficult because it comes from people who love you and are trying to motivate you. A few things that help: recognise that comparison is your parents’ way of expressing concern, not a factual assessment of your worth. Try not to internalise the comparison — your preparation and your exam are specific to you, not relative to anyone else’s. If the comparison is severe and persistent, it is worth naming it directly in a calm moment: “When you compare me to others, it makes me more anxious, not more motivated.” If the anxiety is significant, a therapist can help you develop specific strategies for managing this within your family context.
What is the difference between exam stress and exam anxiety disorder?
Exam stress is a normal, temporary response to academic pressure that typically resolves after the exam or results period. Exam anxiety disorder — formally classified within performance anxiety or social anxiety disorder in the DSM-5 — involves a pattern that is more persistent, more impairing, and not limited to the exam period itself. Students with clinical-level exam anxiety may experience anticipatory anxiety for weeks or months before an exam, may find that anxiety generalises to other performance situations, and may show physical and psychological symptoms that require structured intervention rather than general coping strategies.
External Resources
- World Health Organisation (WHO) — Global prevalence data: anxiety disorders affect 301 million people (2022 Mental Health Atlas)
- American Psychiatric Association / DSM-5 — Diagnostic criteria for GAD, panic disorder, social anxiety disorder
- JAMA Psychiatry — Meta-analysis of CBT efficacy for anxiety disorders; equivalence of online and in-person delivery
- International Journal of Social Psychiatry — Acculturation stress and elevated anxiety/depression rates in South Asian diaspora populations in the UK
- Indian Journal of Psychiatry — Somatisation of psychological distress in Indian clinical populations
- NICE (UK) — Clinical guidelines for the treatment of GAD; first-line recommendations for SSRI/SNRI use
- Transcultural Psychiatry — Acculturation stress and elevated GAD rates in South Asian migrant populations
Struggling?
Talk to an Oppam Therapist
Get the Support You Deserve Online & Confidential