Work stress and burnout Gulf NRIs? He has been in Dubai for eleven years. He sends money home every month without fail — school fees, his parents’ medical bills, the instalment on the house in Thrissur that everyone is proud of. At work he is reliable, careful, always available. His manager has never had cause to complain. But somewhere in the last two years, something changed. He wakes at 4am and cannot get back to sleep. He feels nothing much about anything. The work that once felt meaningful now feels like moving through water. He does not call home as often as he used to because he does not know what to say when his mother asks how he is. He is not sure what the answer is.
Need to Talk to Someone?
Book a private online session with a licensed therapist
This is burnout — not laziness, not ingratitude, not a sign that the Gulf life was a mistake. It is a specific psychological state that develops when chronic workplace stress goes unaddressed for long enough, and it is disproportionately common among Keralite and South Asian NRIs in the Gulf, where the structural conditions of migrant work create a near-perfect environment for its development.
What Burnout Is — and What It Is Not
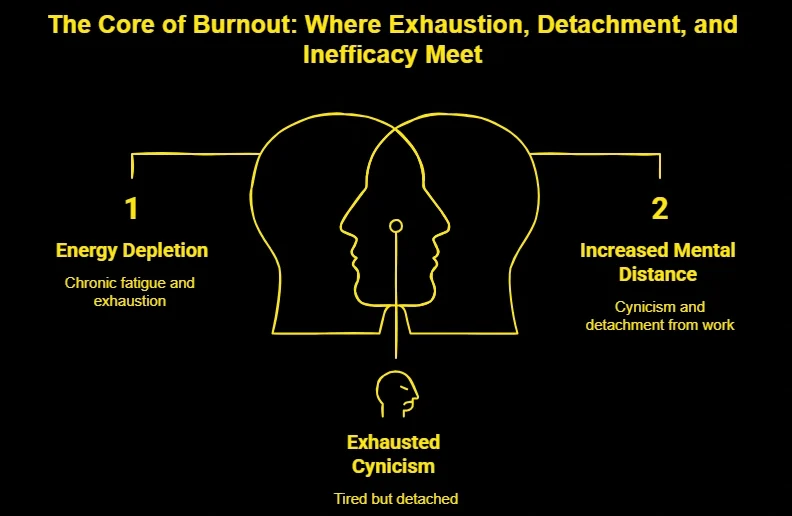
Burnout is not simply being tired after a difficult week. It is a state of chronic depletion — emotional, physical, and cognitive — that results from prolonged exposure to workplace stress without adequate recovery. The World Health Organisation officially recognised burnout as an occupational phenomenon in the ICD-11 in 2019, defining it across three dimensions: feelings of energy depletion or exhaustion; increased mental distance from one’s job, or feelings of negativism or cynicism related to one’s work; and reduced professional efficacy.
work stress and burnout Gulf NRIs
That three-part definition matters because it captures something important: burnout is not just fatigue. It is the specific combination of exhaustion, detachment, and the collapse of the sense that what you are doing is effective or worthwhile. A person can be exhausted and still feel connected to their work. A person can feel cynical without being exhausted. Burnout is when all three converge and persist.
It is also worth distinguishing burnout from occupational stress, which is a normal response to temporary work pressure. Stress, when it resolves, does not cause lasting harm and can even be motivating. The problem arises when stress is chronic, when demands consistently exceed the individual’s resources, and when there is no adequate recovery period. According to research published in the Scandinavian Journal of Work, Environment and Health, the transition from occupational stress to burnout is typically gradual, often taking months or years, which is one reason it is so frequently missed until it is severe
Burnout also needs to be distinguished from depression, though the two conditions overlap and can co-occur. The key clinical distinction is that burnout is primarily work-contextual: the exhaustion and cynicism are most pronounced in relation to work, and the person may experience relief or relative normality in other domains of life. Depression is pervasive — it affects mood, motivation, and engagement across all contexts, not just the workplace. In practice, prolonged burnout frequently tips into depression, which is why early recognition and intervention matter.
Why Gulf NRIs Are Disproportionately Vulnerable
The Gulf is home to one of the largest concentrations of Keralite and South Asian workers in the world. According to data from the Norka Roots department of the Government of Kerala, there are approximately 2.3 million Keralites in the Gulf states, with the UAE, Saudi Arabia, and Qatar hosting the largest numbers. This community is not homogeneous — it includes manual labourers, skilled professionals, healthcare workers, engineers, and business owners — but it shares a set of structural conditions that create elevated risk for work stress and burnout.
The Absence of a Safety Net
In Kerala, stress is managed within a dense social network. Family is physically present. There are neighbours, relatives, the church or mosque community, old friends. When things are difficult, there are people around who notice, who ask, who turn up. In the Gulf, that network is absent or significantly reduced. The NRI worker manages stress largely alone, often in a shared accommodation arrangement that offers limited privacy and little genuine social support.
This social isolation is clinically significant. According to research published in PLOS Medicine by Holt-Lunstad and colleagues, social isolation is associated with a 26 per cent increased risk of mortality and has effects on health outcomes comparable to smoking 15 cigarettes a day. In the context of occupational burnout, isolation removes one of the primary buffers against its development — the ability to decompress, be witnessed, and be supported by people who know you.
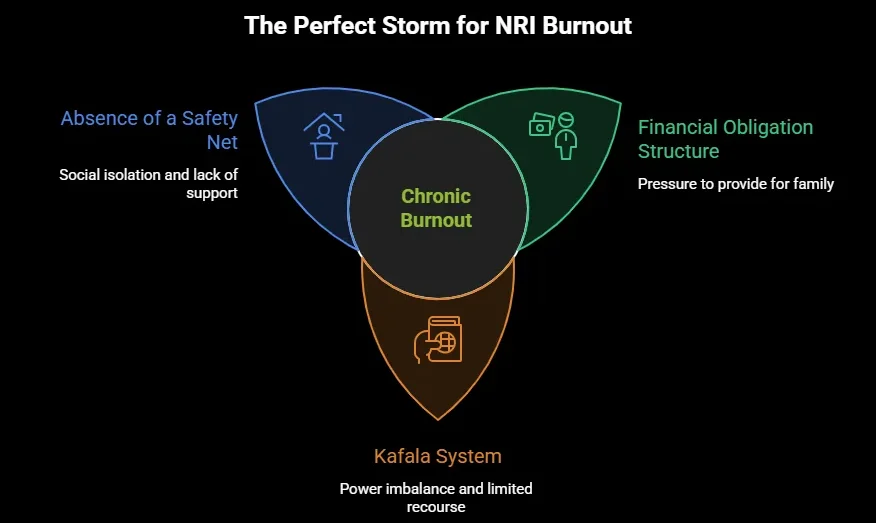
The Financial Obligation Structure
For many Keralite Gulf workers, the purpose of being abroad is explicit and collective: to support the family, to build the house, to fund the children’s education, to care for ageing parents. This is not merely cultural expectation — it is often a genuine financial arrangement that the worker entered into deliberately and feels responsible for maintaining.
The psychological consequence is that rest, boundary-setting, or reducing work hours — all of which are standard recommendations for managing burnout — feel impossible. How do you tell your manager you are overwhelmed when the remittance is what is paying for your father’s cardiac medication? How do you say no to overtime when your family is depending on that extra income? The financial obligation structure that brings Keralites to the Gulf also traps many of them inside unsustainable work patterns from which there is no obvious exit.
The Financial Obligation Structure
In most Gulf countries, the kafala system — the sponsorship model that ties a worker’s legal residency to their employer — creates a structural power imbalance that is a direct contributor to occupational stress. A worker who is mistreated, overworked, or underpaid has limited legal recourse and significant disincentive to complain, because challenging the employer risks not just the job but the right to remain in the country. This power dynamic is a chronic low-level stressor that, when combined with the other conditions described, accelerates burnout considerably.
Recognising Burnout : The Signs That Are Easy to Miss
Understanding the physiology of a panic attack is one of the most effective ways to reduce its power over you.
Physical Signs
Persistent fatigue that does not resolve with sleep or days off is the most consistent physical marker. This is qualitatively different from normal tiredness — it has a heaviness to it, a sense that rest no longer restores. Frequent illness, particularly recurrent infections, reflects the immunosuppressive effect of chronic cortisol elevation. Sleep disturbance — difficulty falling asleep despite exhaustion, or waking in the early hours — is common. So are headaches, digestive problems, and a generalised physical tension that does not fully release.
Psychological Signs
The psychological signs of burnout in Gulf NRIs often manifest as a specific emotional flatness rather than dramatic distress. The person stops caring about things that previously mattered. They go through the motions at work, but the engagement is gone. They feel detached from colleagues, from family phone calls, from the activities that once provided relief. A Keralite worker who used to look forward to his weekly call home, who finds himself avoiding it, making excuses, keeping the conversation short — that withdrawal is a significant signal.
Cynicism is another marker: a persistent sense that the work is pointless, that the organisation does not care, that nothing will change. This is distinct from occasional frustration. It is a settled, joyless scepticism that colours everything.
Behavioural Signs
Behavioural changes include increased use of alcohol or other substances as a coping mechanism, reduced performance at work despite increased effort, social withdrawal, and the abandonment of activities that previously provided pleasure or meaning — exercise, cooking, contact with friends.
Evidence-Based Approaches to Recovery
Acceptance and Commitment Therapy for Burnout
Acceptance and Commitment Therapy has a growing evidence base for occupational burnout. A review published in the Journal of Occupational Health Psychology found ACT-based interventions effective in reducing burnout symptoms, particularly the emotional exhaustion dimension, across multiple workplace contexts.
The core principle most relevant to Gulf NRI burnout is values clarification: identifying what genuinely matters to you, separate from obligation and expectation, and taking small actions in line with those values even within a constrained situation. For a worker whose entire existence has been structured around what he owes others, the question “what do you actually value for yourself?” can be disorienting at first. But it is also, for many people, the beginning of a significant reorientation.
A practical ACT exercise is a brief daily check-in: at the end of each day, note one action you took that reflected something you value — not something you owed, but something you chose. This is not about grand changes to circumstance. It is about introducing small moments of agency and meaning into a life that may feel almost entirely structured by obligation.
Boundaries and Recovery Time
The research literature on burnout consistently identifies the ratio between work demands and recovery resources as the central variable. Recovery in this context does not mean holidays, which are often unavailable or insufficient. It means daily micro-recovery: brief periods during and after work where the person genuinely disengages from work-related concerns.
Research by Sabine Sonnentag at the University of Mannheim, published in the Journal of Applied Psychology, has identified psychological detachment from work during non-work hours as one of the strongest predictors of burnout prevention and recovery. This means not checking work messages after hours, not ruminating about work problems during rest time, and having at least one activity during the day that is genuinely absorbing and work-unrelated.
For Gulf NRIs living in work-heavy environments where social life and work life are often entangled, creating these boundaries requires deliberate effort and sometimes explicit negotiation with employers and housemates. It is not easy. It is, however, clinically meaningful.
Rebuilding Social Connection
Given that social isolation is one of the primary risk factors for burnout in the Gulf context, rebuilding connection—even within the constraints of migrant life— is a genuine intervention rather than a generic wellness recommendation.
This does not require expensive socialising or significant time. It requires regular, genuine contact with people who know you as a person rather than as a function. A weekly video call with a close friend. A regular shared meal with one colleague. Involvement in a community group, however informal. The research on social connection and health, summarised by Holt-Lunstad and colleagues, makes clear that the quality of connection matters more than quantity — one honest conversation is worth more than ten surface-level interactions.
When to Seek Professional Help
Burnout that has been present for more than a few months, that is not responding to self-management strategies, or that has begun to affect domains of life beyond work warrants professional support.
The following signs indicate that individual effort is not enough and that structured clinical input is needed. If you have lost interest in things that have nothing to do with work — hobbies, relationships, the prospect of visiting home — that pervasiveness suggests the burnout has moved into depression. If you are using alcohol or other substances regularly to manage the way you feel, that pattern needs professional attention before it compounds.
For burnout at the severe end of the spectrum without crisis-level symptoms, therapy offers something that self-help cannot: a structured, confidential space to examine the patterns, obligations, and beliefs that have brought you to this point, and to develop a realistic plan for change.
If you are based in India, the Gulf, or anywhere in the South Asian diaspora, Oppam’s therapists can work with you in Malayalam, Tamil, or English, using evidence-based approaches that are adapted to your cultural and personal context. Book your first session →
Frequently Asked Questions
What are the main signs of burnout in NRI workers?
The core signs are persistent exhaustion that does not resolve with rest, emotional detachment or cynicism about work, and a reduced sense of effectiveness — the feeling that effort is no longer producing results. In Gulf NRI workers specifically, these often manifest as emotional flatness, avoidance of family contact, increased irritability, disturbed sleep, and a gradual narrowing of life down to work and little else. Physical symptoms including frequent illness, headaches, and digestive problems are also common. If these have been present for two months or more, a clinical assessment is appropriate.
Is burnout the same as depression?
They overlap but are clinically distinct. Burnout is primarily work-contextual — the exhaustion, detachment, and cynicism are most intense in relation to work, and the person may feel relatively better away from it. Depression is pervasive, affecting mood, motivation, and engagement across all areas of life, including relationships, leisure, and basic functioning. That said, prolonged burnout frequently develops into clinical depression, which is one of the strongest arguments for addressing burnout early rather than waiting to see if it resolves.
Why is burnout so common among Keralites in the Gulf?
Several converging factors are responsible. Social isolation removes the support networks that buffer stress. Financial obligations to family at home prevent the boundary-setting and recovery time that burnout requires. The kafala sponsorship system creates a power imbalance that limits a worker’s ability to challenge poor working conditions. And significant stigma around mental health in Keralite communities means that burnout is often endured silently rather than disclosed and treated. The combination of these factors creates conditions in which burnout can develop and persist for years without being named or addressed.
Can I recover from burnout without taking time off work?
For mild to moderate burnout, yes — though recovery is significantly slower without adequate rest. The evidence-based approach involves improving psychological detachment during non-work hours, rebuilding social connection, introducing regular micro-recovery periods into the working day, and addressing the cognitive patterns that prevent boundary-setting. For severe burnout, time away from work is often clinically necessary and should be discussed with a GP or mental health professional. In the Gulf context, where taking extended leave may feel financially or practically impossible, a therapist can help you identify realistic adjustments within your actual constraints.
Can online therapy help with burnout when I'm based in the Gulf?
Yes, and for Gulf-based workers specifically, online therapy has practical advantages that in-person therapy does not. It removes the need to locate a culturally competent therapist locally, eliminates travel time, and can be scheduled around shift patterns and work hours. Oppam offers sessions in Malayalam, Tamil, and English, which means you can work with a therapist in your first language without the additional effort of translating your experience. Multiple studies have confirmed that online CBT and ACT produce outcomes equivalent to face-to-face therapy for burnout, anxiety, and depression.
How do I explain burnout to my family back home in Kerala?
This is one of the most common practical challenges Gulf NRI workers describe. Families who have not experienced migration stress often struggle to understand how a person can be struggling when they are, by external measures, succeeding. A few approaches that help: frame it in physical terms if that is more comprehensible (“I have been very run down and unwell”); avoid framing it as a choice between family support and your own wellbeing, since that framing tends to increase guilt; and if appropriate, share specific, concrete changes you need — not daily calls when you are too depleted to talk, or a reduction in financial expectations for a defined period. A therapist can help you prepare for these conversations if they feel overwhelming.
What is the difference between work stress and burnout?
Work stress is a normal, often temporary response to high demands. It typically involves feeling pressured, stretched, or overwhelmed, but the person remains engaged and motivated — they want to succeed, they are just finding it difficult. Burnout involves a qualitative shift: the engagement is gone. The person feels not just stretched but empty, not just pressured but indifferent. According to the WHO’s ICD-11 definition, burnout specifically involves exhaustion, cynicism, and reduced efficacy — a combination that distinguishes it from the normal experience of a difficult period at work.
External Resources
-
- World Health Organisation (WHO) — Global prevalence data: anxiety disorders affect 301 million people (2022 Mental Health Atlas)
- American Psychiatric Association / DSM-5 — Diagnostic criteria for GAD, panic disorder, social anxiety disorder
- JAMA Psychiatry — Meta-analysis of CBT efficacy for anxiety disorders; equivalence of online and in-person delivery
- International Journal of Social Psychiatry — Acculturation stress and elevated anxiety/depression rates in South Asian diaspora populations in the UK
- Indian Journal of Psychiatry — Somatisation of psychological distress in Indian clinical populations
- NICE (UK) — Clinical guidelines for the treatment of GAD; first-line recommendations for SSRI/SNRI use
- Transcultural Psychiatry — Acculturation stress and elevated GAD rates in South Asian migrant populations
Struggling?
Talk to an Oppam Therapist
Get the Support You Deserve Online & Confidential